Review Melatonin_Delirium trial
A melatonin-delirium randomized controlled study
By Edward F. Hillenaar, MSc. in medical
March 9, 2023
Introduction
The introduction of this study discusses the issue of postoperative delirium (POD) and its consequences for elderly patients following orthopedic surgery. The occurrence of POD ranges from 3-25% and is linked to prolonged hospitalization, increased mortality and morbidity rates. The study aims to investigate the efficacy of preoperative melatonin administration in reducing POD rates. Melatonin is a hormone produced by the pineal gland and is known to be involved in the regulation of the sleep-wake cycle. Recent research suggests a link between melatonin concentrations in the cerebrospinal fluid and POD after orthopedic surgery. Melatonin is gaining popularity as a way to avoid delirium in hospitalized patients and has been found to be as effective as benzodiazepines in reducing anxiety prior to a procedure without the same side effects. The study hopes to find a drug equivalent to benzodiazepines in anxiolytic efficacy but with fewer side effects.
Methodology and Patients
This is a study of a randomized control clinical trial that was conducted at two hospitals from July to October 2020. The study aimed to evaluate the effects of midazolam and melatonin on delirium symptoms in older adults undergoing surgery. The researchers used systematic random sampling to select 50 patients, and 36 were eligible for the study. The patients were divided into three groups: a control group, a midazolam group, and a melatonin group. The study used the Memorial Delirium Assessment Scale (MDAS) to examine patients 30 minutes, 60 minutes, and 90 minutes after surgery. The follow-up included preoperative assessment of patients’ physical and mental status, monitoring of vital signs and electrolyte levels, and avoiding the use of drug cocktails. The data was analyzed using CHITEST function in Excel and descriptive and analytic statistics by SPSS v.26, with a P-value of less than 0.05 considered statistically significant.
Reviewer’s analysis:
Bargraph of Post Delirium state after 30, 60, and 90 minutes in the three groups (Control, Midazolam and Melatonin)
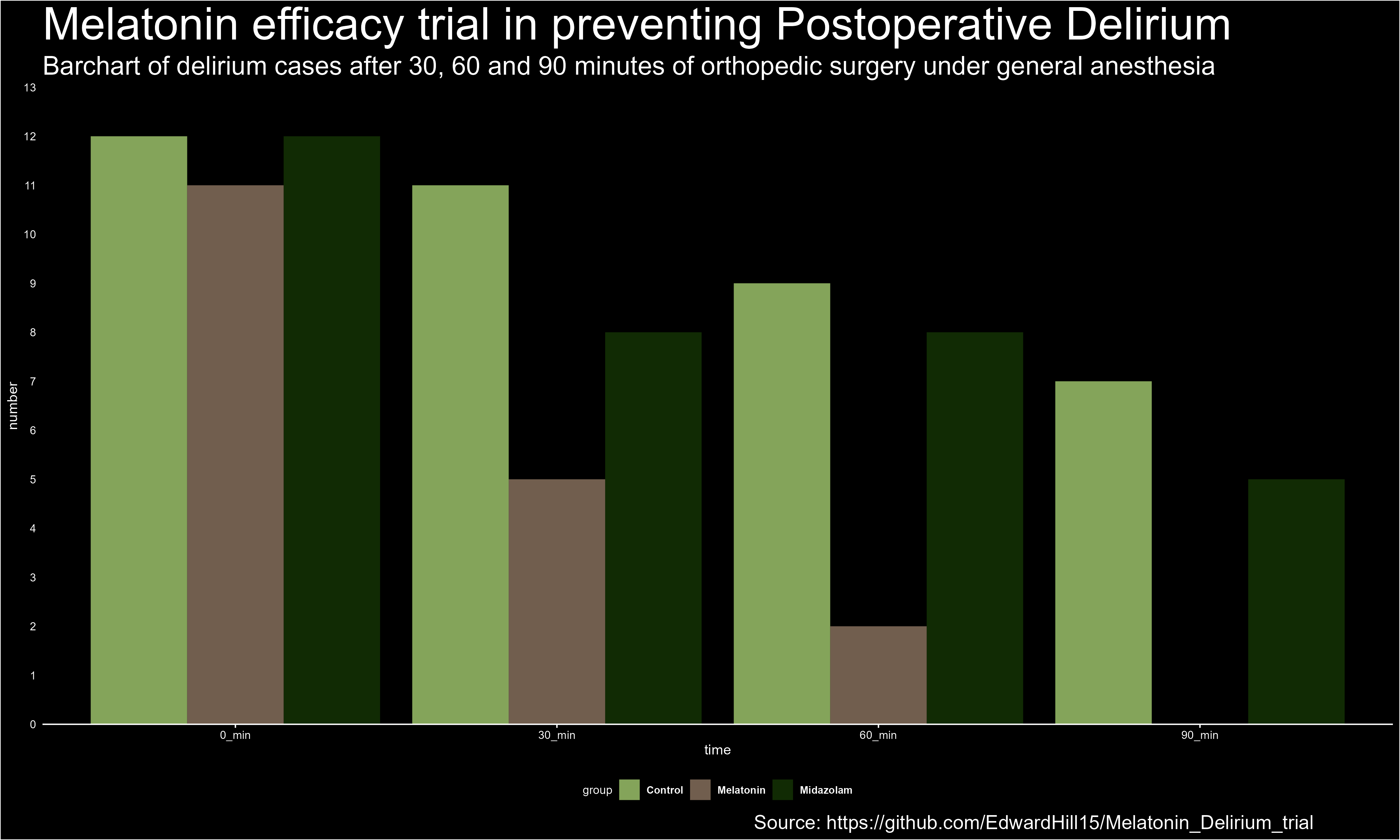
Bargraph of the Delirium-Melatonin study
## Rows: 3 Columns: 5
## ── Column specification ────────────────────────────────────────────────────────
## Delimiter: ";"
## chr (1): group
## dbl (4): n0, n30, n60, n90
##
## ℹ Use `spec()` to retrieve the full column specification for this data.
## ℹ Specify the column types or set `show_col_types = FALSE` to quiet this message.## [1] 3 5## 'data.frame': 3 obs. of 5 variables:
## $ group: chr "Control" "Midazolam" "Melatonin"
## $ n0 : num 12 12 11
## $ n30 : num 11 8 5
## $ n60 : num 9 8 2
## $ n90 : num 7 5 0## group n0 n30 n60 n90
## 1 Control 12 11 9 7
## 2 Midazolam 12 8 8 5
## 3 Melatonin 11 5 2 0## 'data.frame': 12 obs. of 3 variables:
## $ group : Factor w/ 3 levels "Control","Melatonin",..: 1 3 2 1 3 2 1 3 2 1 ...
## $ time : chr "0_min" "0_min" "0_min" "30_min" ...
## $ number: num 12 12 11 11 8 5 9 8 2 7 ...Odss ratios at MDAS measurement 30 minutes after surgery
## delirium30 non-delirium30
## melatonin 5 7
## control 11 1##
## Pearson's Chi-squared test with Yates' continuity correction
##
## data: table1a
## X-squared = 4.6875, df = 1, p-value = 0.03038## Outcome + Outcome - Total Prevalence *
## Exposed + 5 7 12 41.67 (15.17 to 72.33)
## Exposed - 11 1 12 91.67 (61.52 to 99.79)
## Total 16 8 24 66.67 (44.68 to 84.37)
##
## Point estimates and 95% CIs:
## -------------------------------------------------------------------
## Prevalence ratio 0.45 (0.23, 0.91)
## Odds ratio 0.06 (0.01, 0.68)
## Attrib prevalence in the exposed * -50.00 (-81.98, -18.02)
## Attrib fraction in the exposed (%) -120.00 (-338.99, -10.25)
## Attrib prevalence in the population * -25.00 (-49.50, -0.50)
## Attrib fraction in the population (%) -37.50 (-78.85, -5.71)
## -------------------------------------------------------------------
## Yates corrected chi2 test that OR = 1: chi2(1) = 4.688 Pr>chi2 = 0.030
## Fisher exact test that OR = 1: Pr>chi2 = 0.027
## Wald confidence limits
## CI: confidence interval
## * Outcomes per 100 population units##
## Fisher's Exact Test for Count Data
##
## data: table1a
## p-value = 0.02719
## alternative hypothesis: true odds ratio is not equal to 1
## 95 percent confidence interval:
## 0.001331069 0.811072452
## sample estimates:
## odds ratio
## 0.07377038## delirium30 non-delirium30
## midazolam 8 4
## control 11 1##
## Pearson's Chi-squared test with Yates' continuity correction
##
## data: table1b
## X-squared = 1.0105, df = 1, p-value = 0.3148## Outcome + Outcome - Total Prevalence *
## Exposed + 8 4 12 66.67 (34.89 to 90.08)
## Exposed - 11 1 12 91.67 (61.52 to 99.79)
## Total 19 5 24 79.17 (57.85 to 92.87)
##
## Point estimates and 95% CIs:
## -------------------------------------------------------------------
## Prevalence ratio 0.73 (0.47, 1.12)
## Odds ratio 0.18 (0.02, 1.95)
## Attrib prevalence in the exposed * -25.00 (-55.92, 5.92)
## Attrib fraction in the exposed (%) -37.50 (-112.42, 10.99)
## Attrib prevalence in the population * -12.50 (-35.05, 10.05)
## Attrib fraction in the population (%) -15.79 (-40.54, 4.60)
## -------------------------------------------------------------------
## Yates corrected chi2 test that OR = 1: chi2(1) = 1.011 Pr>chi2 = 0.315
## Fisher exact test that OR = 1: Pr>chi2 = 0.317
## Wald confidence limits
## CI: confidence interval
## * Outcomes per 100 population units##
## Fisher's Exact Test for Count Data
##
## data: table1b
## p-value = 0.3168
## alternative hypothesis: true odds ratio is not equal to 1
## 95 percent confidence interval:
## 0.003397033 2.472923285
## sample estimates:
## odds ratio
## 0.1947795## delirium30 non-delirium30
## melatonin 5 7
## midazolam 8 4##
## Pearson's Chi-squared test with Yates' continuity correction
##
## data: table1c
## X-squared = 0.67133, df = 1, p-value = 0.4126## Outcome + Outcome - Total Prevalence *
## Exposed + 5 7 12 41.67 (15.17 to 72.33)
## Exposed - 8 4 12 66.67 (34.89 to 90.08)
## Total 13 11 24 54.17 (32.82 to 74.45)
##
## Point estimates and 95% CIs:
## -------------------------------------------------------------------
## Prevalence ratio 0.63 (0.29, 1.36)
## Odds ratio 0.36 (0.07, 1.88)
## Attrib prevalence in the exposed * -25.00 (-63.59, 13.59)
## Attrib fraction in the exposed (%) -60.00 (-249.00, 26.65)
## Attrib prevalence in the population * -12.50 (-45.80, 20.80)
## Attrib fraction in the population (%) -23.08 (-68.45, 10.08)
## -------------------------------------------------------------------
## Uncorrected chi2 test that OR = 1: chi2(1) = 1.510 Pr>chi2 = 0.219
## Fisher exact test that OR = 1: Pr>chi2 = 0.414
## Wald confidence limits
## CI: confidence interval
## * Outcomes per 100 population units##
## Fisher's Exact Test for Count Data
##
## data: table1c
## p-value = 0.4136
## alternative hypothesis: true odds ratio is not equal to 1
## 95 percent confidence interval:
## 0.04936444 2.44003372
## sample estimates:
## odds ratio
## 0.3734813
Table1a: melatonin vs control at 30 minutes: At 30 minutes after surgery the OR was 0.06 with 95%CI of [0.01, 0.68] when the melatonin group was compared to the control group. That means that the pre-operative administration of melatonin had a significant (p = 0.030) protective effect on post-operative delirium state of consciousness already 30 minutes after surgery.
Table1b: midazolam vs control at 30 minutes: At 30 minutes after surgery the OR was 0.19 with 95%CI of [0.003, 2.473] when the midazolam group was compared to the control group. That means that the pre-operative administration of midazolam had not a significant (p = 0.317) protective effect on post-operative delirium state of consciousness 30 minutes after surgery.
Table1c: melatonin vs midazolam at 30 minutes: At 30 minutes after surgery the OR was 0.37 with 95%CI of [0.049, 2.440] when the melatonin group was compared to the midazolam group. That means that the pre-operative administration of melatonin had not a more significant (p = 0.414) protective effect on post-operative delirium state of consciousness 30 minutes after surgery than the administration of midazolam.
Odds ratios at MDAS measurement 60 minutes after surgery
## delirium60 non-delirium60
## melatonin 2 10
## control 9 3##
## Pearson's Chi-squared test with Yates' continuity correction
##
## data: table2a
## X-squared = 6.042, df = 1, p-value = 0.01397## Outcome + Outcome - Total Prevalence *
## Exposed + 2 10 12 16.67 (2.09 to 48.41)
## Exposed - 9 3 12 75.00 (42.81 to 94.51)
## Total 11 13 24 45.83 (25.55 to 67.18)
##
## Point estimates and 95% CIs:
## -------------------------------------------------------------------
## Prevalence ratio 0.22 (0.06, 0.82)
## Odds ratio 0.07 (0.01, 0.49)
## Attrib prevalence in the exposed * -58.33 (-90.66, -26.01)
## Attrib fraction in the exposed (%) -350.00 (-1562.19, -21.83)
## Attrib prevalence in the population * -29.17 (-60.75, 2.42)
## Attrib fraction in the population (%) -63.64 (-131.80, -15.52)
## -------------------------------------------------------------------
## Uncorrected chi2 test that OR = 1: chi2(1) = 8.224 Pr>chi2 = 0.004
## Fisher exact test that OR = 1: Pr>chi2 = 0.012
## Wald confidence limits
## CI: confidence interval
## * Outcomes per 100 population units##
## Fisher's Exact Test for Count Data
##
## data: table2a
## p-value = 0.01228
## alternative hypothesis: true odds ratio is not equal to 1
## 95 percent confidence interval:
## 0.005239828 0.647345444
## sample estimates:
## odds ratio
## 0.07736941## delirium60 non-delirium60
## midazolam 8 4
## control 9 3## Warning in chisq.test(table2b): Chi-squared approximation may be incorrect##
## Pearson's Chi-squared test with Yates' continuity correction
##
## data: table2b
## X-squared = 0, df = 1, p-value = 1## Outcome + Outcome - Total Prevalence *
## Exposed + 8 4 12 66.67 (34.89 to 90.08)
## Exposed - 9 3 12 75.00 (42.81 to 94.51)
## Total 17 7 24 70.83 (48.91 to 87.38)
##
## Point estimates and 95% CIs:
## -------------------------------------------------------------------
## Prevalence ratio 0.89 (0.53, 1.49)
## Odds ratio 0.67 (0.11, 3.93)
## Attrib prevalence in the exposed * -8.33 (-44.55, 27.88)
## Attrib fraction in the exposed (%) -12.50 (-88.57, 32.88)
## Attrib prevalence in the population * -4.17 (-34.68, 26.34)
## Attrib fraction in the population (%) -5.88 (-35.17, 17.06)
## -------------------------------------------------------------------
## Yates corrected chi2 test that OR = 1: chi2(1) = 0.000 Pr>chi2 = 1.000
## Fisher exact test that OR = 1: Pr>chi2 = 1.000
## Wald confidence limits
## CI: confidence interval
## * Outcomes per 100 population units##
## Fisher's Exact Test for Count Data
##
## data: table2b
## p-value = 1
## alternative hypothesis: true odds ratio is not equal to 1
## 95 percent confidence interval:
## 0.07478974 5.44837199
## sample estimates:
## odds ratio
## 0.6780693## delirium60 non-delirium60
## melatonin 2 10
## midazolam 8 4##
## Pearson's Chi-squared test with Yates' continuity correction
##
## data: table2c
## X-squared = 4.2857, df = 1, p-value = 0.03843## Outcome + Outcome - Total Prevalence *
## Exposed + 2 10 12 16.67 (2.09 to 48.41)
## Exposed - 8 4 12 66.67 (34.89 to 90.08)
## Total 10 14 24 41.67 (22.11 to 63.36)
##
## Point estimates and 95% CIs:
## -------------------------------------------------------------------
## Prevalence ratio 0.25 (0.07, 0.94)
## Odds ratio 0.10 (0.01, 0.69)
## Attrib prevalence in the exposed * -50.00 (-84.00, -16.00)
## Attrib fraction in the exposed (%) -300.00 (-1407.74, -6.12)
## Attrib prevalence in the population * -25.00 (-58.17, 8.17)
## Attrib fraction in the population (%) -60.00 (-128.84, -11.87)
## -------------------------------------------------------------------
## Uncorrected chi2 test that OR = 1: chi2(1) = 6.171 Pr>chi2 = 0.013
## Fisher exact test that OR = 1: Pr>chi2 = 0.036
## Wald confidence limits
## CI: confidence interval
## * Outcomes per 100 population units##
## Fisher's Exact Test for Count Data
##
## data: table2c
## p-value = 0.03607
## alternative hypothesis: true odds ratio is not equal to 1
## 95 percent confidence interval:
## 0.008101526 0.896925044
## sample estimates:
## odds ratio
## 0.1121872
Table2a: At 60 minutes after surgery the OR was 0.08 with 95%CI of [0.005, 0.647] when the melatonin group was compared to the control group. That means that also after 60 minutes there is evidence for a significant protective effect of pre-operative administration of melatonin (p = 0.012) on post-operative delirium state of consciousness.
Table2b: midazolam vs control at 60 minutes: At 60 minutes after surgery the OR was 0.678 with 95%CI of [0.075, 5.448] when the midazolam group was compared to the control group. That means that the pre-operative administration of midazolam had not a significant (p = 1.000) protective effect on post-operative delirium state of consciousness 60 minutes after surgery.
Table2c: melatonin vs midazolam at 60 minutes: At 60 minutes after surgery the OR was 0.11 with 95%CI of [0.008, 0.897] when the melatonin group was compared to the midazolam group. That means that the pre-operative administration of melatonin had a significant (p = 0.036) more protective effect on post-operative delirium state of consciousness 60 minutes after surgery compared to the effect of midazolam on it.
Odds ratios at MDAS measurement 90 minutes after surgery
## delirium90 non-delirium90
## melatonin 0 12
## control 7 5##
## Pearson's Chi-squared test with Yates' continuity correction
##
## data: table3a
## X-squared = 7.2605, df = 1, p-value = 0.007049## Outcome + Outcome - Total Prevalence *
## Exposed + 0 12 12 0.00 (0.00 to 26.46)
## Exposed - 7 5 12 58.33 (27.67 to 84.83)
## Total 7 17 24 29.17 (12.62 to 51.09)
##
## Point estimates and 95% CIs:
## -------------------------------------------------------------------
## Prevalence ratio NaN (NaN, NaN)
## Odds ratio NaN (NaN, NaN)
## Attrib prevalence in the exposed * -58.33 (-86.23, -30.44)
## Attrib fraction in the exposed (%) NaN (NaN, NaN)
## Attrib prevalence in the population * -29.17 (-62.46, 4.13)
## Attrib fraction in the population (%) -100.00 (-198.39, -34.05)
## -------------------------------------------------------------------
## Yates corrected chi2 test that OR = 1: chi2(1) = 7.261 Pr>chi2 = 0.007
## Fisher exact test that OR = 1: Pr>chi2 = 0.005
## Wald confidence limits
## CI: confidence interval
## * Outcomes per 100 population units##
## Fisher's Exact Test for Count Data
##
## data: table3a
## p-value = 0.004577
## alternative hypothesis: true odds ratio is not equal to 1
## 95 percent confidence interval:
## 0.000000 0.449249
## sample estimates:
## odds ratio
## 0## delirium90 non-delirium90
## midazolam 5 7
## control 7 5##
## Pearson's Chi-squared test with Yates' continuity correction
##
## data: table3b
## X-squared = 0.16667, df = 1, p-value = 0.6831## Outcome + Outcome - Total Prevalence *
## Exposed + 5 7 12 41.67 (15.17 to 72.33)
## Exposed - 7 5 12 58.33 (27.67 to 84.83)
## Total 12 12 24 50.00 (29.12 to 70.88)
##
## Point estimates and 95% CIs:
## -------------------------------------------------------------------
## Prevalence ratio 0.71 (0.31, 1.63)
## Odds ratio 0.51 (0.10, 2.59)
## Attrib prevalence in the exposed * -16.67 (-56.11, 22.78)
## Attrib fraction in the exposed (%) -40.00 (-218.73, 38.51)
## Attrib prevalence in the population * -8.33 (-42.66, 25.99)
## Attrib fraction in the population (%) -16.67 (-65.43, 17.72)
## -------------------------------------------------------------------
## Uncorrected chi2 test that OR = 1: chi2(1) = 0.667 Pr>chi2 = 0.414
## Fisher exact test that OR = 1: Pr>chi2 = 0.684
## Wald confidence limits
## CI: confidence interval
## * Outcomes per 100 population units##
## Fisher's Exact Test for Count Data
##
## data: table3b
## p-value = 0.6843
## alternative hypothesis: true odds ratio is not equal to 1
## 95 percent confidence interval:
## 0.07506651 3.35966548
## sample estimates:
## odds ratio
## 0.524988## delirium90 non-delirium90
## melatonin 0 12
## midazolam 5 7##
## Pearson's Chi-squared test with Yates' continuity correction
##
## data: table3c
## X-squared = 4.0421, df = 1, p-value = 0.04438## Outcome + Outcome - Total Prevalence *
## Exposed + 0 12 12 0.00 (0.00 to 26.46)
## Exposed - 5 7 12 41.67 (15.17 to 72.33)
## Total 5 19 24 20.83 (7.13 to 42.15)
##
## Point estimates and 95% CIs:
## -------------------------------------------------------------------
## Prevalence ratio NaN (NaN, NaN)
## Odds ratio NaN (NaN, NaN)
## Attrib prevalence in the exposed * -41.67 (-69.56, -13.77)
## Attrib fraction in the exposed (%) NaN (NaN, NaN)
## Attrib prevalence in the population * -20.83 (-53.11, 11.45)
## Attrib fraction in the population (%) -100.00 (-198.39, -34.05)
## -------------------------------------------------------------------
## Yates corrected chi2 test that OR = 1: chi2(1) = 4.042 Pr>chi2 = 0.044
## Fisher exact test that OR = 1: Pr>chi2 = 0.037
## Wald confidence limits
## CI: confidence interval
## * Outcomes per 100 population units##
## Fisher's Exact Test for Count Data
##
## data: table3c
## p-value = 0.03727
## alternative hypothesis: true odds ratio is not equal to 1
## 95 percent confidence interval:
## 0.0000000 0.8864315
## sample estimates:
## odds ratio
## 0
Table3a: melatonin vs control at 90 minutes: At 90 minutes after surgery the OR was 0 with 95%CI of [0, 0.45] when the melatonin group was compared to the control group. That means that also after 90 minutes there is evidence for a significant protective effect of pre-operative administration of melatonin (p = 0.005) on post-operative delirium state of consciousness.
Table3b: midazolam vs control at 90 minutes: At 90 minutes after surgery the OR was 0.525 with 95%CI of [0.075, 3.360] when the midazolam group was compared to the control group. That means that the pre-operative administration of midazolam had not a significant (p = 0.684) protective effect on post-operative delirium state of consciousness 90 minutes after surgery.
Table3c: melatonin vs midazolam at 90 minutes: At 90 minutes after surgery the OR was 0 with 95%CI of [0, 0.886] when the melatonin group was compared to the midazolam group. That means that the pre-operative administration of melatonin had a significant (p = 0.037) more protective effect on post-operative delirium state of consciousness 90 minutes after surgery compared to the effect of midazolam on it.
Chi Squared Test for the Total Group (N=36)
## delirium non-delirium
## control 7 5
## midazolam 5 7
## melatonin 0 12##
## Pearson's Chi-squared test
##
## data: table_x2
## X-squared = 9.75, df = 2, p-value = 0.007635
Results Chi-Squared Test Total Group:
The results of the Pearson’s Chi-squaerd test of X2 (2, N = 36) = 9.75, p = .0076 indicate that the pre-operative administration of melatonin is dependent on the outcome, i.e., the prevalence of a post-operative state of delirium after surgery. That means that the pre-operative administration of melatonin had a significant effect on reducing a post-operative state of delirium after surgery.
Summary results of reviewer’s analyses
These results are related to odds ratios (OR) at MDAS (Memorial Delirium Assessment Scale) measurement 30 minutes after surgery.
In Table1a, the comparison was made between the melatonin group and the control group. The OR was found to be 0.06, with a 95% confidence interval (CI) of [0.01, 0.68]. This means that the pre-operative administration of melatonin had a significant protective effect (p = 0.030) on post-operative delirium state of consciousness already 30 minutes after surgery.
In Table1b, the comparison was made between the midazolam group and the control group. The OR was found to be 0.19, with a 95% CI of [0.003, 2.473]. This means that the pre-operative administration of midazolam did not have a significant (p = 0.317) protective effect on post-operative delirium state of consciousness 30 minutes after surgery.
In Table1c, the comparison was made between the melatonin group and the midazolam group. The OR was found to be 0.37, with a 95% CI of [0.049, 2.440]. This means that the pre-operative administration of melatonin did not have a significant (p = 0.414) protective effect on post-operative delirium state of consciousness 30 minutes after surgery compared to the effect of midazolam on it.
At 60 minutes after surgery, there is evidence for a significant protective effect of pre-operative administration of melatonin (p = 0.012) on post-operative delirium state of consciousness. However, the pre-operative administration of midazolam had no significant protective effect (p = 1.000) on post-operative delirium state of consciousness 60 minutes after surgery.
Additionally, the pre-operative administration of melatonin had a significant (p = 0.036) more protective effect on post-operative delirium state of consciousness 60 minutes after surgery compared to the effect of midazolam on it.
At 90 minutes after surgery, the odds ratio (OR) for the melatonin group compared to the control group was 0 with a 95% confidence interval (CI) of [0, 0.45], indicating a significant protective effect of pre-operative melatonin administration on post-operative delirium state of consciousness (p = 0.005). However, for the midazolam group compared to the control group, the OR was 0.525 with a 95% CI of [0.075, 3.360], suggesting that pre-operative administration of midazolam did not have a significant protective effect on post-operative delirium state of consciousness (p = 0.684) at 90 minutes after surgery. Additionally, when comparing the melatonin and midazolam groups, the OR was 0 with a 95% CI of [0, 0.886], indicating that pre-operative melatonin had a significantly more protective effect (p = 0.037) on post-operative delirium state of consciousness at 90 minutes after surgery compared to the effect of midazolam.
Finally, a Chi-squared test showed that the administration of melatonin had a significant effect on reducing post-operative delirium. These findings suggest that pre-operative administration of melatonin may be an effective way to prevent post-operative delirium in patients.
Conclusion
Based on the results, it can be concluded that pre-operative administration of melatonin has a significant protective effect on post-operative delirium state of consciousness. This effect was observed as early as 30 minutes after surgery and continued up to 90 minutes after surgery. On the other hand, pre-operative administration of midazolam did not show a significant protective effect on post-operative delirium state of consciousness at any of the measurement times.
Furthermore, when comparing the effect of melatonin to midazolam, melatonin was found to be significantly more effective in protecting against post-operative delirium state of consciousness at both 60 and 90 minutes after surgery.
These findings suggest that melatonin may be a promising option for preventing post-operative delirium state of consciousness, while midazolam may not provide significant benefits in this regard. However, further studies are needed to confirm these findings and to evaluate the long-term effects of melatonin on post-operative delirium state of consciousness.
Discussion
The results of this study suggest that pre-operative administration of melatonin has a significant protective effect on post-operative delirium state of consciousness, whereas pre-operative administration of midazolam did not show a significant protective effect. This effect was observed as early as 30 minutes after surgery and remained significant at 60 and 90 minutes after surgery. Additionally, the protective effect of melatonin was found to be significantly stronger than that of midazolam at 60 and 90 minutes after surgery.
These findings have important clinical implications, as post-operative delirium is a common complication of surgery, especially in elderly patients, and can lead to increased morbidity and mortality. Melatonin, as a natural hormone with sedative and antioxidant properties, may be a safer and more effective alternative to traditional sedatives like midazolam for preventing post-operative delirium.
However, it is important to note that this study has some limitations, including the small sample size and the use of only one dose of melatonin and midazolam. Further research with larger sample sizes and more doses of melatonin and midazolam is needed to confirm these findings and to explore the optimal dose and timing of administration for maximum effect.
In conclusion, the findings of this study suggest that pre-operative administration of melatonin may be an effective way to prevent post-operative delirium, and may be a safer alternative to traditional sedatives. However, further research is needed to confirm these findings and to explore the optimal dose and timing of administration.